
Congress passed a one-time 2.5 percent base pay bump for 2026. CMS quietly blunted it with a structural cut that most practices did not fully model before January 1 arrived. The 2026 Medicare Physician Fee Schedule Final Rule (CMS-1832-F) reduces the indirect practice expense component for facility-based physician services by 50 percent. Combined with a −2.5 percent efficiency adjustment applied to over 7,000 non-time-based CPT codes, a procedure delivered inside a hospital or ambulatory surgical center may absorb a net reimbursement drop of 9 to 10 percent per claim. The political headlines covered the pay bump. They did not hand any specialist a survival plan.
What Exactly Changed in 2026 Medicare Facility Practice Expense?
CMS finalized a 50 percent reduction in the indirect PE RVU component for facility-based physician services under CMS-1832-F, effective January 1, 2026. The policy reduces facility PE allocations tied to work RVUs to half the amount allocated for non-facility services, producing an average 7 percent payment reduction for facility-delivered procedures. Office-based practices received an approximately 4 to 5 percent indirect PE increase under the same redistribution.
The historical logic was baked in decades ago. The Medicare payment formula assumed that physicians billing for facility-based work still maintained separate office practices—paying rent, administrative salaries, and billing overhead out of pocket. That assumption was never revised as physician employment by health systems accelerated. CMS now argues those indirect costs belong to the facility, not the physician, making the legacy PE allocation duplicative.
The conversion factor rose to $33.40 for non-QPP participants and $33.57 for Advanced APM qualifying practitioners, a nominal gain of roughly 3.26 percent. That lift disappears when 50 percent of indirect facility PE evaporates from the formula. Practices relying on high-RVU procedural facility codes that have not yet run a CPT-level impact model against their top 150 billed codes are flying without instruments.
Which Specialties Face the Deepest 2026 Facility PE Losses?
Hematology/oncology physicians practicing in facility settings face an approximate 11 percent reimbursement decrease in 2026, according to ASH analysis, while community-setting oncologists see roughly a 6 percent increase under the same redistribution. Cardiology procedures including pacemaker implants, TAVR, PCI, and catheter ablation face combined RVU reductions of approximately 10 percent. Infectious disease physicians see cuts exceeding 5 percent across 81 percent of their billed codes, per AMA data.
That 17-percentage-point differential between hospital-based and community-based oncologists billing identical CPT codes is the most operationally significant number in CMS-1832-F. It is not a future risk. It is money already absent from January claims.
Internal medicine carries compounding pressure from a different angle. E/M services performed in a facility setting declined in 2026 while the same E/M codes billed from a physician office gained. A full-time hospitalist cannot migrate services. A mixed-setting internist with outpatient office capability sits on recoverable revenue that most practice managers have not yet calculated. Stress tests (CPT 93017) dropped from $311.40 to $220.60 under OPPS restructuring. Amyloid PET (CPT 78803) collapsed from $1,305.48 to $554.73 due to APC reassignment. These are not adjustments. They are structural resets.
How Do Care Management Codes Offset 2026 Facility PE Losses?
Chronic Care Management (CCM, CPT 99490–99491), Principal Care Management (PCM, CPT 99424–99427), and Remote Patient Monitoring (RPM, CPT 99453, 99457–99458) generate recurring monthly revenue with non-facility PE values. These time-based cognitive codes are fully exempt from the −2.5 percent efficiency adjustment and unaffected by the facility PE cut, making them a structurally protected recovery channel for any specialty managing complex chronic patients.
The default assumption—that care management billing requires a separate operational infrastructure—is wrong. A practice already running EHR-based care coordination can activate CCM billing with minimal incremental cost, provided documentation is built into existing clinical touchpoints.
PCM allows practices to target patients with a single high-complexity condition, which is precisely the chronic disease population cardiology and endocrinology already own. An active cardiologist managing 200 complex chronic patients who launches PCM billing can recover $4,000 to $7,000 monthly without adding a single additional encounter, depending on GPCI adjustments. RPM stacks on top. CPT 99457 plus 99458 capture monthly interactive management time with no facility component and generate HEDIS-reportable data that simultaneously strengthens value-based payer negotiations.
How Does Permanent Virtual Supervision Create a Revenue Upside?
CMS permanently adopted virtual direct supervision under 42 CFR §410.32 for diagnostic tests and 42 CFR §410.26 for incident-to services, effective January 1, 2026. The supervising physician or NPP must remain immediately available via real-time, two-way audio-visual technology throughout the service. Audio-only does not qualify. Services tied to 010 or 090 global surgical indicators are explicitly excluded from virtual supervision eligibility.
The throughput upside is operational. Under legacy direct supervision rules, a physician had to be physically present in the procedure suite, capping concurrent diagnostic capacity. Virtual supervision removes that bottleneck. A cardiologist can supervise stress tests across two clinic locations simultaneously through a HIPAA-compliant audio-video platform—doubling throughput without adding physician hours or a second physician salary.
MAC contractors launched post-payment audits targeting virtual supervision compliance immediately in 2026. The OIG has flagged incident-to documentation as a top review priority in its current Work Plan. The permanent rule creates an opportunity. Proper chart documentation is what converts that opportunity into protected revenue.
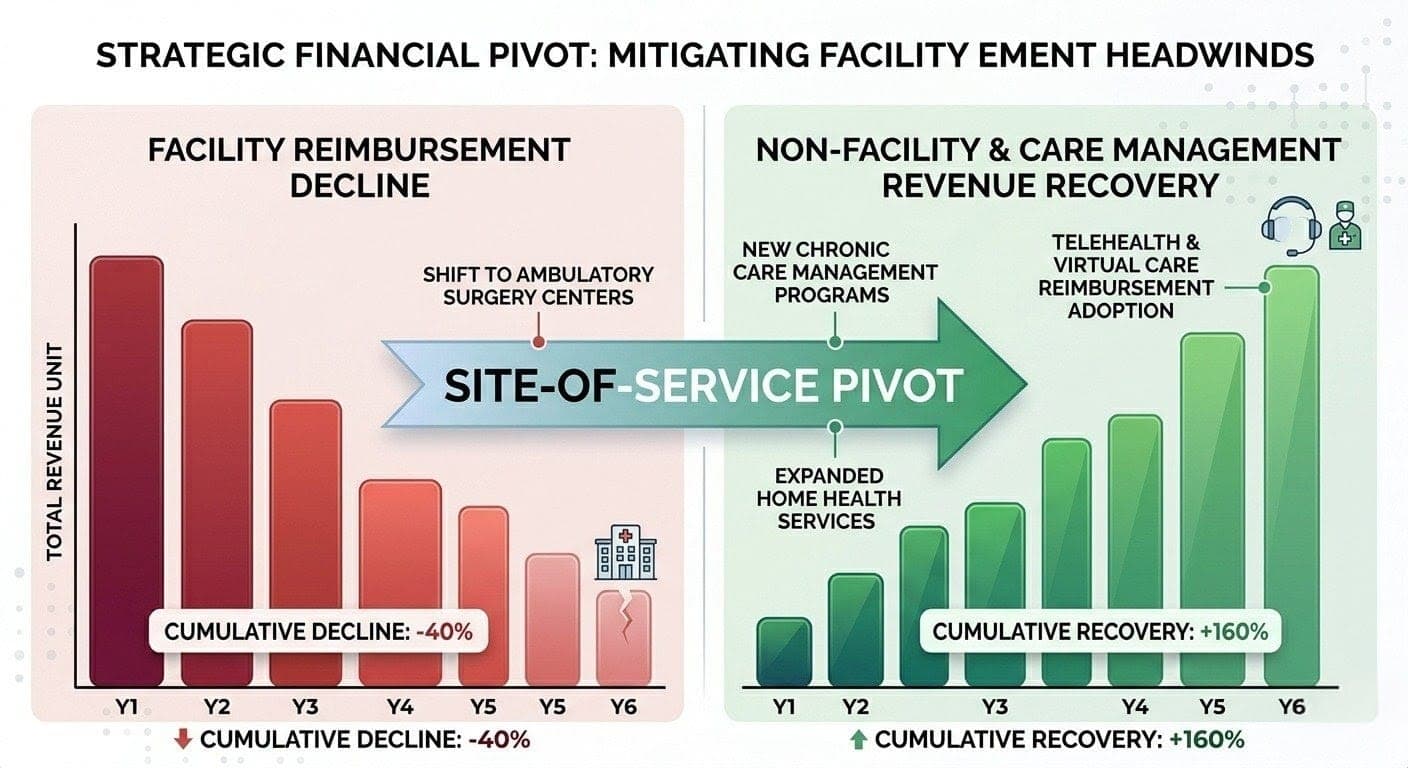
How Do Specialists Execute a Site-of-Service Pivot to Recover Revenue?
Shifting qualifying procedures from hospital outpatient departments (POS 22) to physician office settings (POS 11) applies non-facility PE RVU values, which CMS increased by approximately 4 to 5 percent in 2026. For facility-heavy oncology and internal medicine specialists with in-office infrastructure, a disciplined site-of-service rebalancing can recover 8 to 12 percent of lost Medicare revenue per migrated code—provided clinical feasibility and POS compliance are explicitly verified before the first claim goes out.
Corporate news sites spent Q4 2025 covering the political fallout from CMS-1832-F. None of them gave the oncologist or internist working inside a hybrid practice a step-by-step plan for what to move, when to move it, and where the compliance ceiling sits. Here is that plan.
Step 1: Build a CPT Revenue Differential Map. Pull your top 100 CPT codes by annual claim volume. Cross-reference each code against 2026 MPFS Addendum B for the gap between facility and non-facility payment rates at your MAC’s jurisdiction. Codes with a per-service differential exceeding $30 and annual volume above 150 claims are your primary migration candidates.
For oncologists, infusion administration codes 96413 (chemotherapy, first hour) and 96415 (each additional hour) carry a material non-facility premium when billed from a physician-owned infusion suite versus a hospital outpatient department. For internal medicine, spirometry (CPT 94010), routine EKG with interpretation (CPT 93000), and major joint aspiration or injection (CPT 20610) each carry higher non-facility payment rates and are clinically performable in a properly equipped office setting. For cardiology, Holter monitor interpretation and portable monitoring supervision codes carry non-facility values when the equipment is placed and managed from a physician office location.
Step 2: Assess Clinical and Regulatory Feasibility. Not every code migrates cleanly. Chemotherapy infusion in a physician office requires OSHA-compliant medication storage, emergency equipment, and state licensing verification for drug administration. Confirm that malpractice coverage extends to the proposed office setting for each migrated procedure. Verify that your NPI enrollment lists the office location as an active service site in the Medicare Provider Enrollment, Chain, and Ownership System (PECOS) before billing begins. Billing from an unenrolled location generates denials and triggers post-payment audit flags.
Step 3: Update the Charge Description Master and POS Code Assignments. Every migrated service must carry POS 11 on the claim. It must also actually occur at that location. The Recovery Audit Contractor program maintains open, approved audit topic RAC Issue 0108 specifically for facility-versus-non-facility POS miscoding under the MPFS. A hospital outpatient service billed as POS 11 is not a reimbursement strategy. It is a False Claims Act violation under 31 U.S.C. §3729. There is no gray zone here.
Step 4: Train Charge Capture Staff Before the First Migrated Claim. POS errors originate most frequently at charge entry, not in the coding department. Front-desk and clinical staff must know which services are scheduled at which location before any charge is created. Build location-tagged order sets in your EHR that default POS codes based on the scheduled service site. A manual POS override should require supervisor approval and generate an audit log entry. One systematic error across 400 annual claims creates a repayment demand and OIG exposure that no incremental revenue gain covers.
Can an Advanced APM Shield a Facility-Heavy Practice From Long-Term PE Erosion?
Participation in an Advanced Alternative Payment Model qualifies physicians for the 2026 conversion factor of $33.57 versus $33.40 for non-qualifying practitioners, based on 2024 QP performance data verified at qpp.cms.gov. The CMS Ambulatory Specialty Model, finalized for heart failure and low back pain in 2026, is mandatory for designated practices and creates an episode-based payment structure that bypasses per-service facility PE calculations entirely, removing the site-of-service penalty from the financial equation.
Under bundled payment logic, the total episode payment replaces per-service RVU math. A cardiology practice managing heart failure episodes within the ASM model can capture care coordination fees, shared savings distributions, and quality bonuses that structurally exceed individual PE RVU adjustments—without the facility PE haircut applied to every line item.
The QPP QP determination for 2026 payments was based on 2024 performance data. Practices that failed to confirm QP status before January 1 are locked at the $33.40 rate for the full calendar year. That window has closed. The 2027 preparation cycle is open now, and missing it a second time is not an administrative oversight—it is a compounding financial decision with a defined dollar cost.
The 2026 Medicare facility PE cuts are not a rounding error buried in a 1,800-page rulemaking. They are a structural redistribution that rewards office-based practice and penalizes procedural facility work—with no legislative reversal in sight. Practices that run a CPT-level differential map, launch care management billing, execute a compliance-first site-of-service pivot, and pursue APM alignment will protect margin through this cycle. Those waiting for a CMS course correction may be waiting considerably longer than their cash flow allows.
Leave a Reply