
CMS-0057-F landed in the Federal Register on February 8, 2024, and its January 1, 2026 enforcement deadline has already divided healthcare revenue cycle operations into two camps: organizations that built FHIR-native prior authorization pipelines, and those still faxing X12 278 transactions and waiting on hold with payer call centers.
The gap is financial. CMS projects the rule reduces administrative burden by $15 billion over ten years. That savings belongs to whoever automates first—and becomes a penalty for whoever doesn’t.
This guide targets clinical operations managers, revenue cycle directors, and senior billers who need to audit their own EHR environment, provision API credentials, and run a live FHIR ePA transaction before an auditor asks why denial rates are still climbing.
What Does CMS-0057-F Actually Require From Your Practice in 2026?
CMS-0057-F mandates that Medicare Advantage organizations, Medicaid FFS programs, CHIP, and QHP issuers on the FFE expose FHIR R4 Prior Authorization APIs by January 1, 2026. Standard PA decisions must arrive within 7 calendar days; expedited decisions within 72 hours. Non-compliance triggers Medicare Advantage Star Ratings penalties and CMS corrective action proceedings against impacted payers.
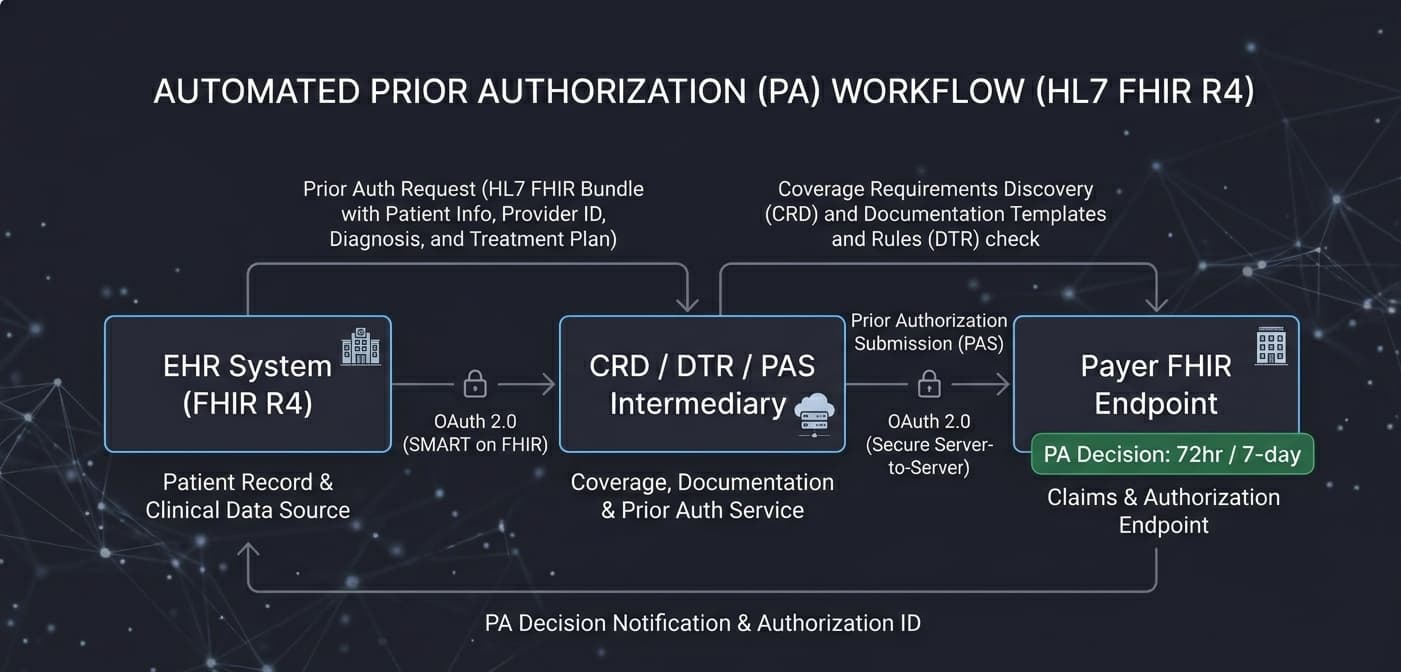
The rule operates on three interlocking HL7 Da Vinci Implementation Guides: Coverage Requirements Discovery (CRD), Documentation Templates and Rules (DTR), and Prior Authorization Support (PAS). CRD fires first, alerting the clinician at point-of-care that prior auth is required. DTR surfaces the exact payer documentation templates inside the EHR. PAS submits a structured FHIR Claim resource to the payer and retrieves a ClaimResponse containing the PA decision—or a pended status requiring follow-up.
What most operational guides miss is a critical structural distinction: CMS compels payers to expose the API. It does not compel your EHR vendor to consume that API without configuration. That gap is where practices get buried.
How Do You Audit Your EHR for FHIR API ePA Readiness?
An EHR FHIR ePA readiness audit requires four sequential checks: confirming FHIR R4 base URL availability, validating SMART on FHIR OAuth 2.0 dynamic client registration support, verifying the Da Vinci PAS STU 2.0.1 capability statement is loaded, and confirming the system can send and receive X12 278 transactions wrapped inside FHIR Bundle resources per the PAS profile.
Begin with your EHR’s FHIR capability statement. Navigate to your base FHIR URL—typically https://[your-ehr-domain]/fhir/R4/metadata—and download the CapabilityStatement JSON. Search for Claim and ClaimResponse under the rest.resource array. If those resource types are absent, or listed without create and search-type interactions, your system cannot process PA transactions natively. You need a middleware layer or a vendor patch.
The second checkpoint is OAuth 2.0 client registration. Every payer FHIR endpoint requires your EHR to present a valid Bearer token per API call. In Epic, SMART on FHIR configuration sits under Security > SMART on FHIR Applications. In Oracle Health (Cerner), it lives in the Millennium API Management Console. Confirm your system supports dynamic client registration per RFC 7591. Static credentials provisioned manually per payer create a maintenance disaster at scale.
Third, verify your PAS Implementation Guide version. PAS STU 2.0.1 is the operative version for CMS-0057-F compliance. Earlier STU 1.x builds use deprecated Claim profile structures that fail validation against payer endpoints enforcing IG conformance. Ask your vendor directly whether their PAS capability statement includes the canonical URL http://hl7.org/fhir/us/davinci-pas/CapabilityStatement/capability-statement-pas-intermediary-server. If they can’t answer, escalate.
Which EHR Configurations Block Token-Based Auth Handshakes?
Three EHR configurations consistently block OAuth 2.0 token exchange with payer FHIR endpoints: outbound HTTPS traffic filtered at the application firewall without payer IP allowlisting, misconfigured SMART launch context scopes—particularly missing system/Claim.write and system/ClaimResponse.read—and expired or absent client certificates in the TLS mutual authentication layer required by some Medicare Advantage payers.
The firewall problem is the most overlooked blocker in independent practices. FHIR payer endpoints operate on port 443 but sit on domains your network security team has never whitelisted. Obtain every payer’s FHIR endpoint base URL from their developer portal before the first live call—CMS maintains a partial registry, but MA plans publish their own. Feed those domains to your network team and verify bidirectional HTTPS clearance.
Scope misconfiguration is the silent revenue killer. Without system/Claim.write, every POST to the payer’s FHIR server returns 403 Forbidden—and your staff will chase a ghost that looks like a connectivity problem. That misdiagnosis costs hours.
How Does the FHIR Prior Auth Workflow Execute Step-by-Step?
The FHIR ePA workflow executes in five sequential API calls: (1) the order-sign CDS Hook fires a CRD service call at order entry; (2) DTR launches a SMART app to populate required documentation; (3) PAS submits a FHIR Claim Bundle to the payer intermediary; (4) the EHR polls the ClaimResponse endpoint; (5) the PA decision writes back into the encounter record, closing the authorization loop automatically.
Step three is where revenue cycle risk concentrates. The PAS FHIR Claim Bundle must carry correct DiagnosisSequence, ProcedureSequence, and SupportingInfo slices per the Da Vinci PAS profile. A missing required slice—particularly supportingInfo:admissionDates for inpatient submissions—triggers a synchronous rejection from the payer intermediary, not a pended status. Your workflow logic must parse ClaimResponse.outcome precisely: complete means approved, queued means pended, error means rejected with a named OperationOutcome.
Per MGMA’s 2023 Prior Authorization Survey, practices spend an average of 14 staff hours per physician per week on prior auth. A properly configured FHIR PAS workflow reduces that to minutes. A single misconfigured Bundle slice rebuilds the entire queue.
What Happens When a Payer FHIR Endpoint Returns a 401 or 429 Error?
A 401 Unauthorized response means the Bearer token is expired, the client ID is unrecognized, or the requested OAuth scopes exceed what the payer authorized during client registration. A 429 Too Many Requests response indicates a rate-limit breach; most Medicare Advantage payer FHIR endpoints enforce limits between 60 and 100 API calls per minute per registered client ID.
OAuth 2.0 access tokens issued by payer authorization servers typically carry a 300-second TTL. If your EHR does not implement proactive token refresh before expiry, every workflow spanning more than five minutes fails silently mid-call. That failure surfaces as a missing PA record three days later—after the service has already been rendered.
Rate limiting demands exponential backoff logic. A linear retry loop burns your rate budget and risks client suspension. Implement a backoff starting at two seconds, doubling per retry, capped at five retries. Log every 429 with the Retry-After header value and surface rate limit events to your operations dashboard. Recurring 429s against a single payer endpoint signal that your volume is hitting plan-level caps that require a vendor escalation call, not a developer fix.
What Are the Financial and Compliance Risks of Skipping FHIR ePA Implementation?
Practices that delay FHIR-based ePA face three compounding risk vectors: elevated claim denial rates averaging 5–10% of gross revenue per HFMA benchmarks, False Claims Act exposure when services render without documented PA approval, and CMS audit flags triggered when procedure codes requiring prior auth carry no corresponding PA documentation in the claim record.
The False Claims Act exposure is not speculative. Under 31 U.S.C. § 3729, submitting a claim for a service rendered without proper prior authorization—when that auth was denied or never obtained—constitutes a false claim if the provider knew or should have known prior approval was required. The DOJ recovered $2.68 billion in healthcare fraud judgments and settlements in FY2023 alone. PA documentation gaps appear routinely in OIG Work Plan audit targets.
At an average reimbursement of $1,200 per inpatient claim, a 6% denial rate across 500 monthly claims represents $36,000 in monthly revenue at risk—before accounting for rework labor. The AMA reports 94% of physicians describe prior auth as causing direct delays in care access, a metric CMS cited explicitly in the CMS-0057-F preamble as primary justification for the mandate.
How Do You Validate CMS-0057-F Compliance Before the Enforcement Deadline?
CMS-0057-F compliance validation requires three documented operational tests: a successful end-to-end PAS transaction against a payer sandbox returning a ClaimResponse with outcome “complete,” a SMART on FHIR token exchange log showing valid scope grants, and an internal audit trail confirming PA decisions are stored in the EHR within the 7-day standard and 72-hour expedited turnaround windows.
Run your PAS workflow against at least three payer sandbox environments before going live. Test the rejection path explicitly: submit a Claim Bundle with a deliberately missing required slice and confirm your error-handling logic parses the OperationOutcome correctly and routes the case to a manual review queue rather than dropping it silently. Silent failures are the single greatest operational risk in FHIR ePA implementations.
Document every test. CMS auditors examining CMS-0057-F compliance will request evidence of implementation due diligence. Maintain a compliance log recording the payer FHIR endpoint URL tested, test date, ClaimResponse outcome, error codes encountered, and remediation actions taken. That log is your primary defense artifact if a prior auth documentation dispute escalates to a federal investigation.
Engage your clearinghouse as a structural accelerant. Availity Essentials and Waystar both offer FHIR ePA intermediary services that normalize transaction flow across multiple payer endpoints simultaneously—eliminating per-payer configuration overhead. Neither service replaces the need to audit your EHR’s token handling and scope configuration, but both absorb the endpoint variability that makes multi-payer FHIR rollouts operationally fragile without in-house developer resources.
The January 2026 deadline is not a calendar event on the horizon. It is an active operational gap. Every practice still running prior authorization through a staff member on hold with a payer is paying an administrative tax that FHIR automation eliminates—and absorbing liability exposure that a properly configured API workflow closes permanently.
Leave a Reply