
Three words define the highest-exposure compliance liability in healthcare billing right now: copy, paste, forward. What started as an EHR shortcut has become the primary target of Recovery Audit Contractors, Targeted Probe and Educate reviewers, and OIG program integrity contractors. Modern EHR audit trail technology strips providers of plausible deniability. Auditors can detect cloning algorithmically, at scale. The question is whether your organization has built controls to stop it before they arrive.
Why Is Copy-Paste Documentation the Most Audited Behavior in Medicare Billing Right Now?
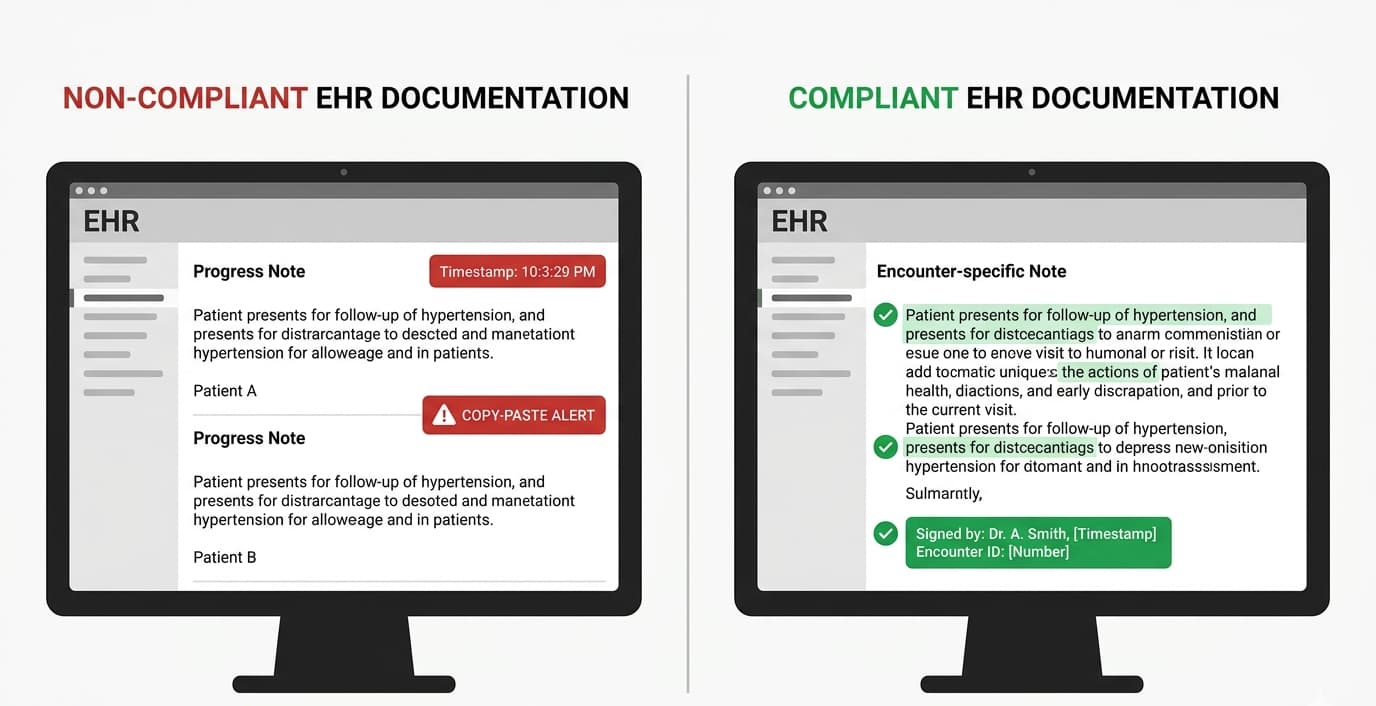
Copy-paste documentation, known as cloning, creates identical or near-identical records across separate patient encounters. CMS and OIG identify cloning as a primary mechanism for improper E/M payments and upcoding under Medicare and Medicaid. In 2026, EHR metadata — creation timestamps, modification logs, and field-level audit trails — allows federal contractors to detect cloned entries with algorithmic precision across large claim cohorts.
The OIG sounded the formal alarm in its 2013 hospital audit. It found that only 25% of surveyed facilities maintained copy-paste policies. That governance gap didn’t shrink. It compounded as EHR adoption accelerated. RAC contractors now cross-reference modification timestamps against submitted claim profiles. A note created at 9:04 a.m. with zero subsequent edits, carrying a high-level E/M code, is a pattern. Patterns trigger automated flags.
The financial arithmetic is brutal. HFMA data places per-claim rework cost at $25. A cloning-triggered RAC audit doesn’t produce one denial. It reopens an entire claim cohort spanning multiple review periods. That is before any False Claims Act exposure enters the calculation.
What Does CMS Define as Cloned Documentation Under Current E/M Standards?
CMS defines cloned documentation as any record where the clinical narrative, examination findings, or medical decision-making is identical or near-identical across multiple encounters — regardless of the patient’s presenting condition or clinical trajectory. This includes copied-forward histories, auto-populated templated exams without provider verification, and physician attestations mirroring prior notes without encounter-specific modification or clinical rationale.
A nuance most guides miss: CMS’s 2021 E/M revisions permit review-and-verify attestation for medical history. Providers may state they reviewed prior documentation and confirmed its accuracy. What they cannot do is carry forward clinical judgment elements — COPA, MDM, or treatment plan — unchanged when the clinical picture has shifted. The 2026 E/M framework determines level of service exclusively by MDM or total time. That places maximum audit weight on the clinical reasoning documented under MDM — exactly where cloning creates catastrophic exposure. Outsource Strategies
A provider treating a COPD patient whose condition improved by day four of inpatient admission, but whose copied MDM still reflects acute admission complexity, has produced a record that cannot defend its billing level. Ventra Health’s clinical reviews documented this exact pattern in hospital medicine settings.
How Does Copy-Paste Documentation Create False Claims Act Liability?
Cloned documentation creates False Claims Act liability when billing Medicare or Medicaid for services at a higher complexity level than the encounter supported. DOJ and courts applying Universal Health Services v. Escobar (2016) treat systematic cloning as constructive knowledge of documentation inaccuracy. That eliminates good-faith ignorance as a defense. It satisfies both the materiality and scienter standards required for FCA liability.
OIG alleged that Somerset Medical Center’s cardiology group knowingly presented claims for services it knew or should have known were not provided as claimed — a standard applied directly to cloned E/M progress notes submitted for higher-level services than actually rendered. Physicians Practice
Federal civil penalties currently run from $13,946 to $27,894 per false claim. Treble damages apply to the full overpayment. A mid-volume practice submitting 2,000 inflated E/M claims annually faces theoretical eight-figure exposure before the first settlement negotiation. EHR logs showing note creation timestamps with zero provider modification, followed immediately by high-level claim submission, eliminate the ignorance argument in most federal circuits. Audit trail metadata is government evidence. Treat it accordingly.
What Operational Controls Actually Stop Copy-Paste Cloning at Its Source?
Eliminating copy-paste documentation risk requires four controls applied in sequence: a formal written EHR policy mandating attribution and encounter-specific modification; EHR configuration restricting auto-population of clinical judgment fields; automated documentation similarity scoring within the platform; and mandatory provider education tied directly to denial trends and code distribution analysis rather than generic compliance training.
The policy layer sets the legal baseline. The AMA and CMS recommend that organizations ensure copied or pasted information is accurate, up-to-date, relevant to the current encounter, and compliant with organizational policies — with the rendering provider personally accountable for the finalized record. American Medical Association
At the configuration level, Epic’s SmartText and Oracle Health’s Discern toolsets allow administrators to restrict clinical field auto-population. They can require attestation checkboxes before note finalization. They can trigger alerts when content similarity exceeds defined thresholds. Most practices leave these native controls undeployed. That is a zero-cost defense left on the table. (CMS Medicare Program Integrity Manual, Chapter 3: cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/pim83c03.pdf)
How Should a Compliant Policy Define Permissible Note Carry-Forward?
A compliant attribution policy requires providers to identify copied content by source encounter date, confirm the rendering provider reviewed and verified its clinical accuracy for the current visit, and document the specific clinical basis for why prior information remains applicable today. Blanket review-and-verify language without encounter-specific clinical support does not satisfy CMS program integrity standards or withstand RAC review.
Attribution language is a legal shield. “HPI reviewed from 04/15/2026; patient confirms no interval symptom change, verified via today’s direct assessment” survives scrutiny. A verbatim HPI copy with no modification timestamp does not. Build attestation into note finalization workflows at the EHR level so it cannot be bypassed under time pressure.
What Does a 2026-Ready Internal Audit Protocol Look Like for Cloned Note Detection?
A 2026-compliant internal audit protocol includes monthly random sampling of the top 20% of E/M billers by volume, EHR audit log review comparing note creation and modification timestamps, documentation similarity scoring across consecutive encounters for the same provider-patient pair, and quarterly scorecards correlating documentation patterns with E/M code distribution outliers and payer denial rates.
RAC contractors and MAC auditors do not read notes manually. They run pattern-matching analytics. Your internal audit must mirror that approach. Pull 20 consecutive notes from a high-volume provider. Compare HPI language, MDM assessments, and COPA documentation across encounters. The OIG Work Plan continues to include audits focused on improper payments driven by outdated or inconsistent records. Similarity rates above 70% without documented clinical justification represent an exposure that must be corrected before an external contractor identifies it first. AAPC
Prioritize the highest-risk specialties. Inpatient hospitalist medicine, pain management, behavioral health, and cardiology appear on OIG’s radar annually. Pair documentation audits with CPT distribution analysis. Any provider whose billing clusters heavily at 99215 or 99285 without corresponding MDM complexity is a primary external review target. (OIG Work Plan: oig.hhs.gov/reports-and-publications/workplan)
How Do You Fix Cloned Documentation Without Destroying Physician Productivity?
Eliminating copy-paste risk without damaging physician efficiency requires replacing cloning workflows with AI-assisted ambient documentation tools. These tools generate encounter-specific notes from recorded physician-patient dialogue. Paired with structured templates that auto-populate only non-clinical administrative fields, they reduce documentation time while producing notes that are encounter-specific and audit-defensible by design.
The productivity objection is legitimate. The AMA’s 2024 Physician Practice Benchmark Survey documents an average of 15 hours per week on administrative documentation. Copy-paste survives because it works in the short term. It stops working the moment a RAC cohort review reopens two years of claims.
Ambient scribing platforms — Nuance DAX Copilot, Abridge, and Suki — generate structured clinical notes from captured encounter dialogue. The resulting documentation reflects what was said in that room on that day. Not the prior visit. Not the prior admission. Health systems deploying these tools report documentation time reductions of 25% to 50%, alongside measurable improvement in note specificity. CMS and Medicare contractors now use analytics to identify billing behaviors disconnected from documentation quality. Encounter-specific notes are not just a compliance requirement. They are a revenue protection mechanism. Billingmedtech
Reframe the conversation with providers. Connect documentation accuracy to cash flow. A cloned note triggering a RAC denial costs the claim value, the $25 rework expense, and the cumulative audit risk of the entire flagged cohort. That is a financial conversation. It is the only kind that consistently changes physician behavior.
The 2026 enforcement environment has removed ambiguity. CMS requires encounter-specific documentation that independently supports every billed service. OIG contractors have the infrastructure to detect cloning at scale. Federal courts read systematic cloning as constructive knowledge of false billing. Practices treating this as a policy problem will keep reacting to audits. Those treating it as an operational and financial priority will build controls that protect their revenue cycle — and their continued participation in federal healthcare programs.
This article reflects regulatory guidance current as of May 2026. Consult qualified healthcare compliance counsel before implementing documentation policy changes.
Leave a Reply