

Let me be direct with you. Every denied claim is not just a billing inconvenience. It is lost revenue, wasted staff time, and in many cases, a patient who ends up caught in the middle.
I have seen practices lose hundreds of thousands of dollars annually, not from bad medicine, but from fixable billing gaps. The industry finally has the data to prove it — and the tools to fix it.
What Is Claim Denial Management, Exactly?
Claim denial management is the systematic process of identifying, analyzing, appealing, and preventing insurance claim denials within a healthcare
revenue cycle. It covers both reactive appeals and proactive prevention strategies to protect a provider’s financial health.
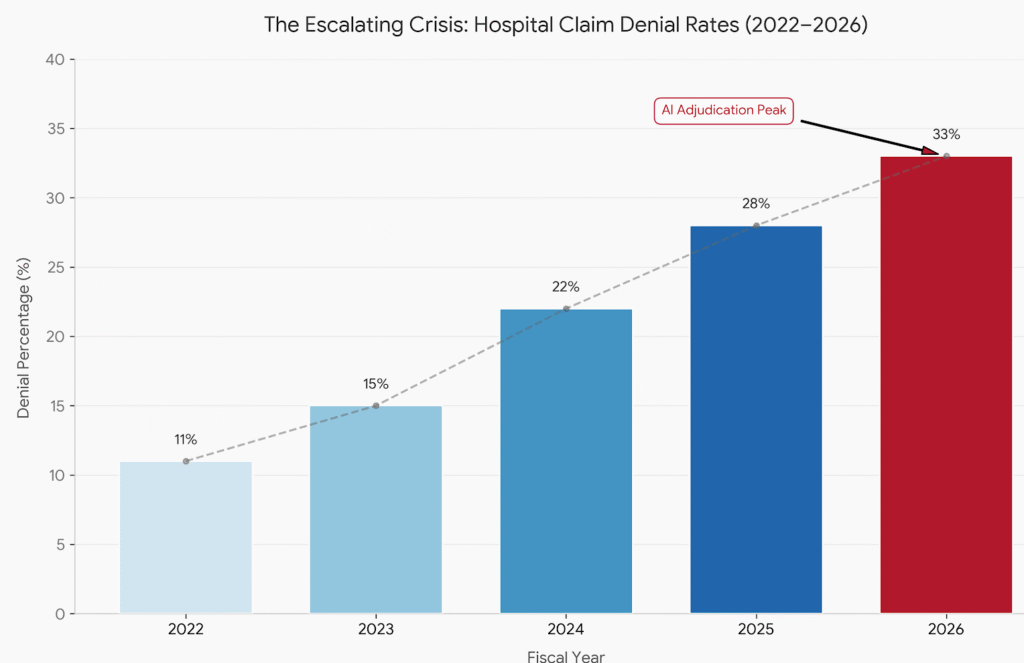
Why Are Denial Rates Still Rising in 2026?
The numbers are hard to ignore. Initial claim denial rates hit 11.8% in 2024, up from 10.2% just a few years earlier. In 2025, 41% of providers now report denial rates above 10% — the highest figure since tracking began in 2022, according to Experian Health’s State of Claims report.
Three forces are driving this surge:
Payers are using AI offensively. Insurers now deploy machine learning to review claims at scale. This speeds up denials without proportionally speeding up approvals.
Regulatory complexity is compounding. The No Surprises Act, prior authorization reforms, and evolving Medicare Advantage rules have all added layers of compliance risk to every claim submitted.
Front-end data errors persist. A striking 76% of denials trace back to missing, incomplete, or inaccurate data — problems that exist before a claim ever reaches the payer.
Meanwhile, commercial plan denials rose 1.5% and Medicare Advantage denials jumped 4.8% between 2023 and 2024. This is not a niche problem. It is an industry-wide revenue crisis.
What Are the Most Common Reasons Claims Get Denied?
The top causes of claim denial are missing or inaccurate patient data, lack of prior authorization, incorrect coding, eligibility issues, and medical necessity disputes. These five categories account for the vast majority of preventable denials across all payer types.
Here is where most practices bleed revenue:
- Eligibility failures — Insurance details were not verified in real time before the visit.
- Authorization gaps — Services were rendered without required pre-approval, especially under Medicare Advantage plans.
- Coding errors — ICD-10 or CPT mismatches, often worsened by annual code updates.
- Duplicate submissions — Resubmitting before a payer responds creates automatic rejections.
- Medical necessity denials — Vague or incomplete clinical documentation fails to justify the service.
What separates high-performing practices is not that they never make these errors. It is that they catch them before submission.
How Much Does a Denied Claim Actually Cost You?
The administrative cost per denied claim rose from $43.84 in 2022 to $57.23 in 2023 — a 30% jump in just one year. Multiply that across thousands of annual claims and the math becomes unsettling.
HFMA research shows hospitals lose an average of 4.8% of net revenue to denials. For a large health system, that translates to tens of millions of dollars annually. The Advisory Board estimates that proactive denial prevention can recover up to $10 million per $1 billion in patient revenue.
And the hidden cost? Staff burnout. Ninety percent of denied claims require manual rework. That is repetitive, demoralizing work — and a major driver of turnover inside revenue cycle teams.
Is AI Actually Helping With Claim Denial Management?
It depends on which “AI” you are talking about — and that distinction matters more than most vendors will tell you.
Among the small group of providers (just 14%) currently using AI for denial management, 69% report it has reduced denials or improved resubmission success. Those results are real. But they largely come from large health systems with the data volume and infrastructure to support genuine machine learning. The picture looks different for smaller practices.
The labeling problem you need to know about
Most tools marketed as “AI-powered” to small and mid-size practices are rules-based engines — sophisticated claim scrubbers that flag a missing modifier, a blank field, or a mismatched payer ID. That is useful. It is not machine learning. It does not adapt when a payer quietly shifts its prior authorization criteria for a specific CPT code mid-year.
True ML-based denial prediction learns from remittance outcomes across tens of thousands of claims. It identifies which payer-code combinations are trending toward denial before your billing team notices the pattern. That capability requires high claim volume — typically 50,000 or more annually — clean structured data, and continuous retraining as payer behavior shifts. Most small practices simply do not generate that volume independently.
What this means for small practices
A solo practitioner or small group submitting 8,000 to 12,000 claims per year cannot train a meaningful proprietary model. When a vendor promises AI-driven denial prediction at that scale, ask them directly: what was the model trained on, how often does it retrain, and what is the minimum claim volume it requires? If they cannot answer clearly, you are buying a rules engine with better marketing.
The most practical path to genuine ML value for smaller organizations is through a third-party RCM partner that pools claims data across many practices. Aggregated datasets restore the volume needed for predictive accuracy — but only if that aggregator has sufficient claims within your specialty and regional payer mix. A model trained on urban oncology data will not reliably predict denial behavior under a rural BCBS contract.
The Deloitte Center for Health Solutions found that automated claim scrubbing and predictive validation — including both rules-based and ML approaches — can prevent up to 85% of avoidable denials and reduce administrative cost per claim by nearly 25%. That figure holds at scale. For small practices, the honest priority is clean claim scrubbing and real-time eligibility verification first, with ML-backed prediction accessed through an aggregated platform rather than a standalone tool.
What Does a Proactive Denial Prevention Strategy Look Like?
A strong denial prevention strategy combines clean front-end intake, real-time eligibility checks, pre-submission claim scrubbing, payer-specific coding rules, and a dedicated appeals workflow with root-cause tracking. Prevention costs far less than rework.
Start here:
1. Fix the front end first. Patient registration and insurance verification are where most denials originate. Real-time eligibility checks at scheduling — not just at check-in — catch problems before the appointment ever happens.
2. Centralize prior authorization workflows. Authorization management should be tracked in one system, not scattered across staff members’ inboxes. Automate reminders and expiration alerts.
3. Conduct quarterly coding audits. CPT codes change annually. Payer-specific rules change even more often. Scheduled audits with certified coders catch patterns before they become systemic denial trends.
4. Build a denial tracking dashboard. You cannot fix what you do not measure. Track denial rates by payer, denial code, provider, and service line. Look for patterns — not just individual errors.
5. Create a formal appeals process. Most providers appeal fewer than 10% of denied claims. Yet the MGMA notes that nearly two-thirds of denials are recoverable with the right workflow. A structured, timely appeals process is leaving money on the table if it is absent.
Should You Outsource Denial Management or Keep It In-House?
Outsourcing denial management works best for organizations without dedicated revenue cycle staff, high denial volumes, or recurring coding complexity. In-house teams offer more control and institutional knowledge, but require consistent training and the right technology stack.
A small orthopedic practice in Texas reduced its denial rate from 18% per month to significantly lower figures within one year of partnering with a specialized billing service — after implementing structured denial tracking, real-time eligibility checks, and coder retraining. The lesson: the right support structure matters more than the insourcing-versus-outsourcing label.
How Do You Measure Denial Management Success?
Track these key performance indicators every month:
| Metric | Target Benchmark |
|---|---|
| Clean claim rate | 95%+ |
| First-pass acceptance rate | 90%+ |
| Denial rate | Below 5% |
| Appeal success rate | 60%+ |
| Days to resolution | Under 30 days |
Any metric consistently outside these ranges signals a systemic gap — not a one-off error.
For deeper benchmarking, the American Health Information Management Association (AHIMA) offers peer-reviewed guidance on revenue cycle performance standards: AHIMA Revenue Cycle Resources
What Should Small Practices Prioritize First?
Small practices should prioritize real-time eligibility verification and clean claim submission above all else. These two steps address the majority of preventable denials without requiring large technology investments or additional staff.
The return on even basic automation is immediate. One missed prior authorization can cost more than an entire month of a software subscription.
The Gap Most Competitors Miss
Most articles on this topic focus exclusively on appeals — the reactive end of the process. But the real opportunity lies upstream.
Prevention is always cheaper than appeals. A claim that never gets denied costs $0 to manage. A denied claim costs $57.23 minimum — and climbs from there with every appeal cycle, staff hour, and payer phone call.
The practices winning this game are treating denial management as a quality control function, not a billing department function. They involve clinicians in documentation review. They give schedulers denial-trend data. They tie coding accuracy to performance conversations.
That mindset shift is what separates a 3% denial rate from a 12% one.
Final Thought
Claim denial management is not an administrative nuisance. It is a clinical and financial discipline that touches every part of a healthcare organization — from front desk staff to the CFO.
The data is clear. Denials are rising. Costs are compounding. And the technology to reverse this trend exists today.
The practices that will thrive are not waiting for denials to arrive and then scrambling to appeal them. They are building systems that make the clean claim the default — not the exception.
Start with your data. Find your top three denial codes. Work backwards. Fix the root cause.
That is how you win.
Sources: Experian Health State of Claims 2025 | HFMA Revenue Cycle Data | Deloitte Center for Health Solutions 2024 | MGMA Benchmarking Report 2024 | American Journal of Managed Care 2025 | Advisory Board 2024
Leave a Reply