
Why Are POS 02 and POS 10 Errors the Fastest-Growing Source of Telehealth Claim Denials in 2026?
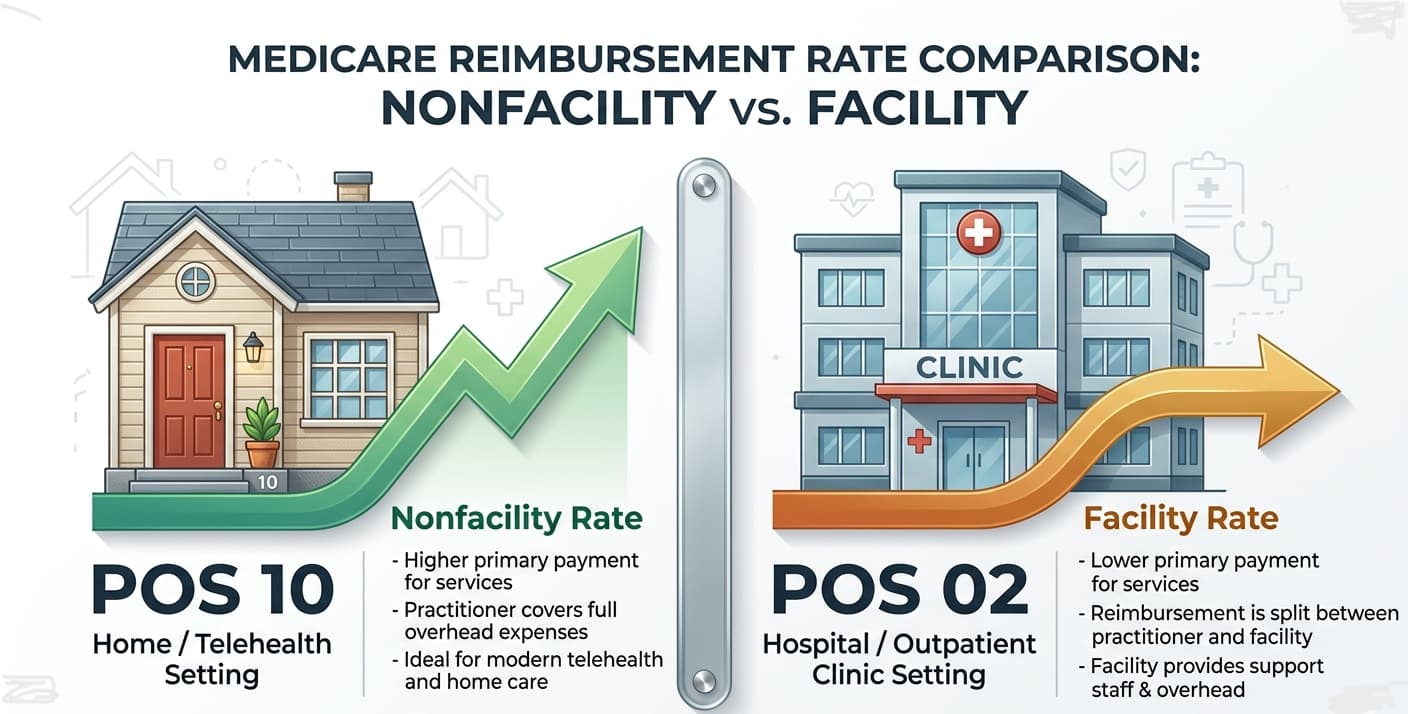
POS misclassification between POS 02 (telehealth not in the patient’s home) and POS 10 (telehealth in the patient’s home) is the most consequential billing error in virtual care today. In 2026, this distinction determines whether a claim pays at the nonfacility rate, silently underpays at the facility rate, or triggers a payer audit flag for documentation inconsistency.
The volume problem is structural. The global telehealth market surpassed USD 186 billion in 2025 and is accelerating toward a projected USD 1.27 trillion by 2034. Every percentage point of POS misclassification across that volume compounds into eight-figure revenue leakage at scale. Most practices do not see it coming.
Clearinghouses pass these claims as technically clean. The POS code is valid, the modifier is attached, the CPT is covered. The damage lands on the remittance, not the rejection queue. That invisible failure mode is where 2026’s denial landscape has become particularly punishing — and where generic guidance leaves revenue teams most exposed.
What Did CMS Change About POS Code Reimbursement Logic in the 2026 Physician Fee Schedule?
The CMS-1832-F Final Rule, effective January 1, 2026, raised physician reimbursement 3.85 percent — the first increase after five consecutive cuts — while exempting telehealth services on the Medicare Telehealth Services List from the new negative 2.5 percent RVU efficiency adjustment applied to non-time-based codes. Correct POS assignment has never been more financially decisive.
The originating site facility fee rose to $31.85 for CY2026, up from $31.01. CMS also streamlined the Medicare Telehealth Services List review process, eliminating the provisional/permanent code distinction and clarifying the two-way interactive audio-video standard that governs which services qualify. Critically, the Consolidated Appropriations Act of 2026 extended several COVID-era telehealth flexibilities, but only through January 30, 2026 for non-behavioral services at Rural Health Clinics and Federally Qualified Health Centers. Practices that failed to track that cliff date generated a concentrated spike in POS-related rejections in February 2026 when those extended rules expired mid-billing cycle.
The compliance pressure compounds. Billing teams already navigating the modifier obsolescence of GT in most Medicare claims — while Modifier 95 governs synchronous audio-video encounters and Modifier 93 covers audio-only — are simultaneously absorbing post-extension deadline recalibrations across multiple payer grids. Error rates climb precisely when documentation workflows are most disrupted.
How Much Revenue Does a Single POS 02 vs. POS 10 Miscoding Actually Cost Per Claim?
For a 99214 Medicare telehealth encounter in 2026, using POS 02 when the patient was home yields the facility rate (~$84.50) instead of the nonfacility rate (~$135.61) — a $51.11 loss per claim. For a behavioral health 90837, the gap is approximately $42. A practice miscoding 30 percent of 20 daily home-based sessions loses over $90,000 annually.
These are not denials. They are underpayments. No CARC code fires. No rejection appears in the clearinghouse dashboard. The practice receives payment, reconciles against the remittance, and if it lacks payment variance analysis, moves on. That reconciliation gap is where most revenue disappears — invisibly, and at scale.
Hard denials — where a payer returns the claim with a rejection remark — occur when POS 02 is billed for a patient clearly documented in the EHR as home-based and the payer’s claim-editing system flags the contradiction. Silent underpayments occur when the incorrect POS code aligns with no obvious contradiction but triggers the wrong reimbursement logic. Both are preventable. They require different interventions. Hard denials need appeal workflows and documentation correction. Silent underpayments need retrospective payment variance audits — a process most revenue cycle teams do not run systematically.
Identifying the underpayment pattern after three months of claims data is what separates high-performing RCM operations from average ones. For mental health billing specifically, practices running 90837 sessions at scale — a common high-volume scenario in behavioral health groups — should calculate their POS-adjusted revenue gap monthly using CMS Physician Fee Schedule Look-Up Tool data to quantify exposure before it accumulates.
What Does the Clinical Record Need to Prove Patient Location for a POS 02 or POS 10 Claim?
CMS telehealth guidance requires the clinical record to confirm patient location at time of service. POS 10 requires documentation that the patient connected from a private home. POS 02 requires confirmation of a non-home setting. The POS code in CMS-1500 Box 24B must align exactly with the encounter note, intake record, and scheduling system location field.
This three-point consistency — claim, note, scheduling record — is where audit exposure concentrates. OIG’s expanded telehealth oversight, embedded in its 2025–2026 Work Plan, specifically targets billing patterns where POS codes contradict clinical documentation. AI-powered analytics deployed by CMS and commercial payers now cross-reference claims data against structured and unstructured clinical note fields at scale.
A provider whose scheduling system defaults all telehealth visits to POS 02 — a common EHR configuration error inherited from legacy implementations — while notes consistently reference home-based patient locations generates a systematic documentation conflict. Modern payer audit algorithms surface this pattern rapidly. It is not a coder training problem. It is an EHR configuration problem that requires direct remediation at the system level.
The False Claims Act exposure here is concrete. In Q1 2026, the DOJ established the National Fraud Enforcement Division specifically to pursue healthcare billing fraud with expanded analytical resources. FCA liability carries treble damages plus civil monetary penalties per false claim. For a high-volume telehealth practice with systemic POS miscoding, aggregate exposure can far exceed the revenue the miscoding generated. CMS telehealth billing guidance is available at cms.gov/Medicare/Medicare-General-Information/Telehealth.
How Do Commercial Payer POS Rules Diverge from CMS, and Where Do Denial Rates Spike?
CMS provides the definitional framework for POS 02 and POS 10, but commercial payers adjudicate these codes against proprietary telehealth coverage grids that regularly diverge from Medicare logic. Some plans require POS 02 even for home-based encounters when the CPT appears on their facility-only telehealth schedule. Others apply parity rules that equalize rates regardless of POS code.
This commercial payer variance is the most operationally dangerous gap in 2026 telehealth billing. UnitedHealthcare, Aetna, and regional BCBS plans each maintain payer-specific telehealth eligible services lists. Billing a CPT code that a specific payer does not cover via telehealth — regardless of correct POS coding and Modifier 95 attachment — generates a hard denial because the service is not a covered benefit in that modality. The list is payer-specific, not universal, and it updates annually.
Behavioral health carve-outs compound this further. Where a member’s mental health benefits are administered by a separate insurer from the primary plan, POS codes must be evaluated against two distinct coverage grids simultaneously. Filing a claim to the medical plan instead of the carve-out administrator generates a hard denial that cannot be resubmitted to the original payer; it must be refiled with the correct entity before that plan’s separate timely filing window closes. At that point, denial often becomes permanent revenue loss.
CMS permanently authorized Medicare coverage for audio-only behavioral health telehealth in 2026. That change created a new modifier decision tree. Audio-only sessions require Modifier 93, not 95, and POS 10 still applies when the patient is at home. Practices that auto-apply Modifier 95 to all behavioral telehealth claims — a workflow inherited from COVID-era blanket approvals — now generate a specific category of technical denials on audio-only sessions that require modifier-level correction rather than simple resubmission.
What Three Workflow Changes Eliminate POS 02 vs. POS 10 Denial Exposure at the Root?
Systematic POS error elimination requires intervention at three distinct operational nodes. At scheduling, intake workflows must capture patient location as a structured data field — not a free-text note — before the encounter begins. At documentation, EHR templates must include a mandatory clinician-confirmed location attestation. At claim editing, clearinghouse scrubbing rules must include POS-versus-note consistency checks as a mandatory pre-submission validation layer.
The scheduling system fix carries the highest ROI. Most POS errors originate in EHR default settings configured at implementation and never audited. When a system defaults all telehealth visits to POS 02 regardless of patient location, every home-based encounter becomes a silent underpayment until that default is corrected. Clearinghouses — Availity, Change Healthcare, Office Ally — offer configurable pre-submission audit rules that catch this mismatch before claims transmit. Any practice running more than 50 telehealth encounters per week should treat POS validation as a mandatory scrub layer.
Quarterly retrospective POS audits against ERA remittance data are equally non-negotiable. These audits surface underpayment patterns that never generate denials — the silent revenue drain that standard denial management dashboards miss entirely. OIG’s telehealth compliance resources, including enforcement alerts and Work Plan priorities, are available at oig.hhs.gov/reports/featured/telehealth.
The practices dominating telehealth revenue cycle performance in 2026 are not the ones with the lowest denial rates. They are the ones that have closed the underpayment visibility gap — because that is where the real money is hiding.
YMYL Disclosure: This article addresses medical billing regulations and compliance requirements that directly affect healthcare revenue and legal obligations. All regulatory references reflect the CMS-1832-F Final Rule (CMS-1832-F) effective January 1, 2026, and the Consolidated Appropriations Act of 2026. Consult a certified professional coder (CPC), healthcare attorney, or RCM compliance specialist before implementing billing workflow changes.
Leave a Reply