 By Eman Zahra
By Eman Zahra
The 2026 billing environment arrived with more structural pressure than most revenue cycle teams projected. The current CMS NCCI 2026Q2 table, effective April 1, 2026, contains over 3.1 million active PTP code-pair rules. Alongside that, the mandatory TEAM bundled payment model went live January 1, covering hip, knee, and femur episodes across selected geographies. The combination is not incremental complexity — it is a structural shift that punishes every practice still running on annual compliance reviews instead of quarterly operational audits. OrbDoc
What Are CMS Overlapping Services Bundling Rules in 2026?
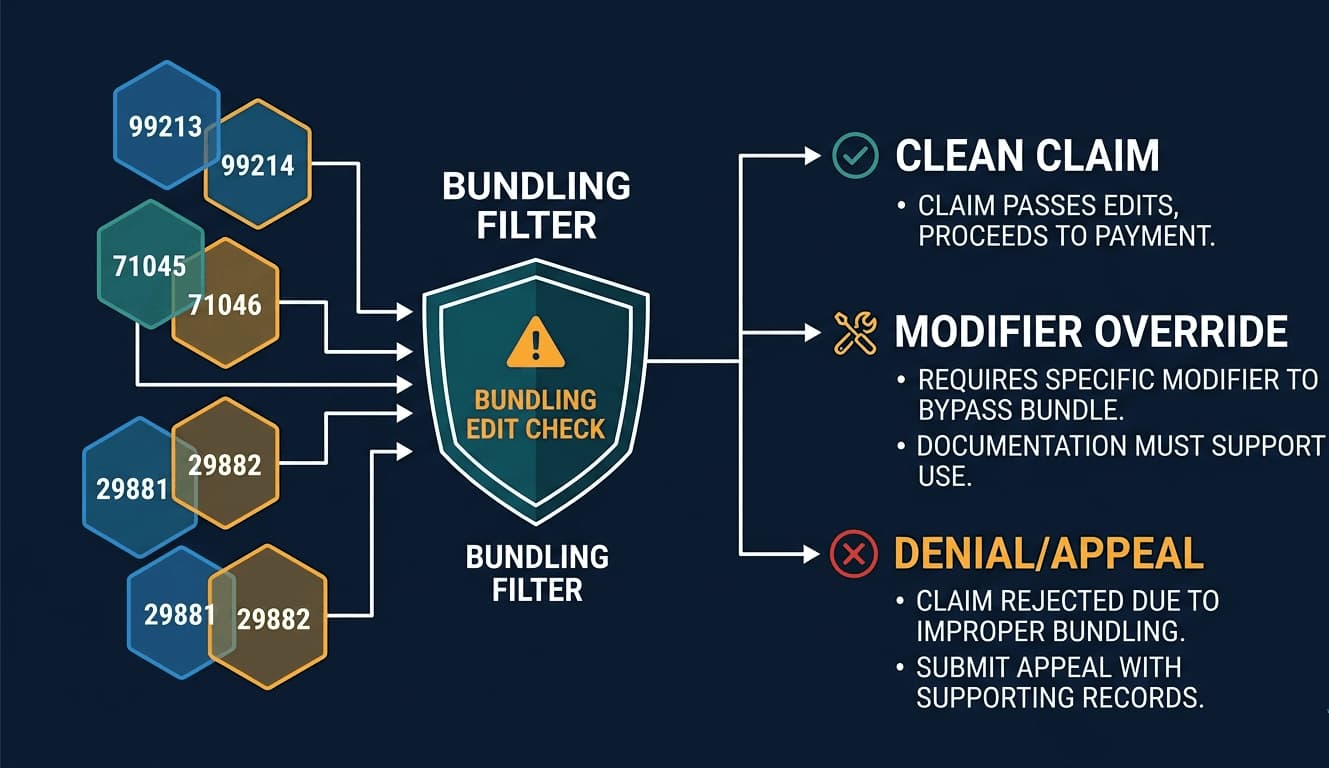
CMS overlapping services bundling rules in 2026 are a set of payment policies — enforced through NCCI Procedure-to-Procedure (PTP) edits, Medically Unlikely Edits (MUEs), and global surgical package provisions under the Medicare Physician Fee Schedule — that prohibit separate reimbursement for services clinically considered components of a more comprehensive procedure billed on the same date of service.
The architecture is layered and unforgiving. At its foundation, PTP edits are built on the comprehensive/component principle: when a larger service is performed, all integral component procedures are bundled and cannot be billed separately. Documentation guidelines are critical, as providers must support any instance where separate payment is necessary even when procedures would generally be considered bundled services. MedStates
Above PTP edits sit MUEs, which cap the billable units of any single code per patient per date. Neither table is static. CMS updates NCCI edit files every quarter — January, April, July, and October. A code combination that cleared Q4 2025 scrubbing can fail a Q1 2026 claim without any change to clinical practice. Practices that rely on annual compliance reviews absorb those denials silently, eroding net collection rates while never identifying the root cause. Coding Ahead
Why Do NCCI Edits Keep Evolving — and What Changed in 2026?
NCCI edits evolve quarterly because CMS continuously realigns payment policy with clinical practice standards. Key 2026 changes include expanded TEAM bundled payment model enforcement for hip, knee, and femur episodes; heightened RAC scrutiny on Modifier 59 usage; tightened MUE limits on high-volume surgical code pairs; and ongoing global surgery accuracy recalibration under the MACRA-mandated data collection initiative.
The TEAM model launched January 1, 2026, replacing the legacy CJR program in selected geographies and tying hip, knee, and femur reimbursement to 30-day episode performance. That 30-day window creates a direct structural collision with the 90-day global surgical package. Practices managing orthopedic volume in TEAM-participating MSAs must now track overlapping obligations across two distinct payment architectures simultaneously. 247medicalbillingservices
On global surgery, CMS’s CY 2026 rule acknowledged that only about 28 percent of expected post-operative visits are actually being performed, while the bundled payment structure still compensates as if 100 percent occur. Beginning January 1, 2025, modifier -54 became mandatory whenever the surgeon will not provide follow-up care, and CMS created HCPCS code G0559 to reimburse other practitioners who deliver post-operative visits. The 2026 rule retained and extended both policies. Practices with split post-operative care arrangements that have not built G0559 into their charge capture logic are billing incorrectly today. Holland & Knight
What Is the Real Financial Risk of a Bundling Violation?
A CMS bundling violation carries three tiers of financial exposure: immediate claim denial generating CO-97 remittance adjustments; post-payment recoupment via RAC, SMRC, or MAC review when a systematic pattern is identified; and potential False Claims Act liability if unbundling is deemed intentional, carrying civil monetary penalties up to three times the overpayment amount plus per-claim fines exceeding $20,000.
The OIG has kept Modifier 59 misuse on its Work Plan for multiple consecutive years. An OIG review found that 40 percent of code pairs billed with Modifier 59 failed to meet program requirements. That figure predates the 2026 tightening of RAC and SMRC review activity on modifier misuse patterns. A practice billing 500 claims per month with a 5 percent Modifier 59 error rate carries not just denial exposure — it carries pre-payment review risk that can freeze reimbursement across the entire provider number. LegalClarity
Revenue leakage runs in the opposite direction too. Practices that over-bundle — declining to bill legitimately separate services out of audit fear — forfeit recoverable revenue on every claim. The compliance mandate runs bidirectionally, and that is the nuance most bundling guides miss entirely.
How Does the Global Surgical Package Create Hidden Overlap Traps?
The Medicare global surgical package bundles pre-operative, intraoperative, and post-operative services into a single procedure payment covering 0, 10, or 90 days. Any evaluation and management service billed within that window for the same related condition automatically denies without appropriate modifiers — primarily Modifier -24, -25, -54, -57, or -79 — depending on the specific clinical and timing circumstances.
Roughly 15 to 20 percent of orthopedic E/M denials trace back to missed Modifier -24 or -79 applications on otherwise legitimate claims. The operational failure is systemic: the front-end billing team was never alerted that a global period was active when the charge was entered. 247medicalbillingservices
The fix is architectural. Build a global period flag into the practice management system that fires whenever any provider within the group bills an E/M against a patient with an active global period under the same tax ID. That single workflow intercepts the majority of CO-97 denials generated during 90-day surgical windows. Without the flag logic, coders apply modifiers reactively after denial — wasting time on appeals that a pre-submission scrubber would have prevented. [See: CMS Medicare Claims Processing Manual, Chapter 12 — cms.gov/regulations-and-guidance/guidance/manuals]
Which Modifier Strategy Actually Protects Against NCCI Denials in 2026?
In 2026, correct modifier strategy requires selecting the most specific applicable modifier before defaulting to Modifier 59. CMS prefers the X{EPSU} subset modifiers — XE (separate encounter), XP (separate practitioner), XS (separate structure), and XU (unusual non-overlapping service) — and auditors increasingly flag claims where Modifier 59 was used when a more precise X modifier clearly applied.
Modifier 59 remains valid and acceptable, but as of 2026, CMS auditors increasingly scrutinize whether a more descriptive X modifier would have been more appropriate. The modifier choice is not administrative discretion — it is a documented clinical assertion. XS applies to services performed at anatomically distinct sites in the same operative session. XP applies when two providers in the same group each deliver a separate service to the same patient on the same date. Using the wrong one is a compliance failure that a payer audit will surface. Coding Ahead
Documentation must support the modifier selected. Appending XS to a claim where the operative note describes a single anatomical site exposes the practice to a recoupment demand, not just a denial. Quarterly internal audits should sample modifier usage against clinical documentation as a standing RCM function — not an annual exercise. [See: AAPC guidance on CMS X{EPSU} modifier implementation — aapc.com]
How Should RCM Teams Build a 2026 Bundling Compliance Workflow?
RCM teams should implement a five-layer 2026 bundling compliance workflow: quarterly NCCI PTP and MUE file updates integrated directly into the practice management system; pre-submission code-pair scrubbing via clearinghouse or AI-assisted bundling tool; global period flag logic embedded at the EHR charge capture layer; modifier decision trees built into coder review; and monthly denial root-cause analysis segmented by CARC code.
With 3.3 million edit pairs updated quarterly, it is literally impossible for billing staff to check manually — the compliance challenge scales beyond human capacity without automated detection. Practices running manual edit-checking absorb preventable denials every cycle and only discover systematic patterns months after the revenue loss has compounded. BillAudit AI
CO-97 — “payment included in the allowance for another service” — is the specific CARC that isolates NCCI bundling denials from other remittance adjustments. CO-97 indicates that the billed service is already included in the payment for another service rendered on the same day. It is the most common NCCI-related denial code. Segmenting denials by this code, then tracing back to the originating code pair and the modifier applied — or not applied — generates an actionable remediation dataset. If a team cannot name the top five code pairs generating CO-97 denials in the trailing 90 days, the compliance program is reactive by design. U Control Billing
The 2026 bundling landscape will not stabilize. CMS continues to recalibrate PTP edits and global surgery payment methodology simultaneously, while TEAM and emerging episode-based payment models introduce accountability windows that extend well beyond single-claim compliance. The organizations that navigate this environment without revenue loss are not the ones that understand the rules — they are the ones that operationalize the rules into daily workflow before the next quarterly NCCI file drops.
Leave a Reply